
 Lumbar spine stenosis is most common in middle age and the elderly.Symptoms include pain in the lower back and lower extremities, limited movement, numbness and tingling , weakness. Most cases of lumbar stenosis is caused by degenerative and arthritic changes in the intervertebral discs, ligaments and the facet joints surrounding the lumbar canal. Men are affected more so than women. CT scans with or without intrathecal contrast is one diagnostic way to find stenosis. However,MRI is better at viewing soft tissue, the cauda equina, spinal cord, ligaments , epidural fat, subarachnoid space and intervertebral discs. Decompressive lumbar laminectomy is the surgical treatment for lumbar stenosis.This is a serious surgery with risks. Although around ninety five percent of patients find some level of relief and consider this to outweigh the risk. Lumbar bracing, bed rest, physical therapy and pain management are the non surgical treatments.
Lumbar spine stenosis is most common in middle age and the elderly.Symptoms include pain in the lower back and lower extremities, limited movement, numbness and tingling , weakness. Most cases of lumbar stenosis is caused by degenerative and arthritic changes in the intervertebral discs, ligaments and the facet joints surrounding the lumbar canal. Men are affected more so than women. CT scans with or without intrathecal contrast is one diagnostic way to find stenosis. However,MRI is better at viewing soft tissue, the cauda equina, spinal cord, ligaments , epidural fat, subarachnoid space and intervertebral discs. Decompressive lumbar laminectomy is the surgical treatment for lumbar stenosis.This is a serious surgery with risks. Although around ninety five percent of patients find some level of relief and consider this to outweigh the risk. Lumbar bracing, bed rest, physical therapy and pain management are the non surgical treatments.Figures 4A and 4B . (Left) Unenhanced T1-weighted axial magnetic resonance scan at a lumbar level showing severe stenosis. The combination of ligament and facet joint hypertrophy concentrically reduces the diameter of the lumbar canal. The significant reduction in the relative amount of epidural fat and subarachnoid cerebral spinal fluid signal is further evidence of the degree of canal stenosis. (Right) Unenhanced T1-weighted sagittal magnetic resonance scan of the lumbosacral spine showing severe canal stenosis at the L4-5 level, produced by a combination of disc herniation, spondyloarthritis and posterior element hypertrophy. Compare this stenosis with the moderate degree of stenosis observed at levels above. Mild spondylolisthesis is also evident at L5-S1. Magnetic Resonance Imaging
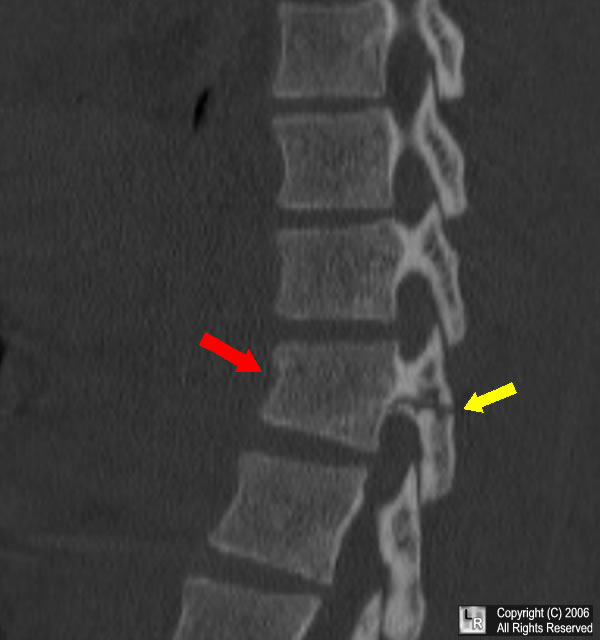 This is an image of a reformatted sagittal CT image of the lower thoracic spine. There is a horizontal fracture through the spinous process and pedicles. There is also a compression fracture of the vertebral body. These types of injures are seen in impact injures where hyperflexion has occured with lap seatbelt injuries. It is also seen in certain types of falls. The most common symptom is back pain. Half of the patients with this type of injury also have serious blunt injury to their internal organs. These are usually lower level of t-spine so spinal cord injury is rare. However, spinal nerve damage is common resulting in bowel and bladder problems. Treatment of these fractures are done with immobilization and surgical fixation.
This is an image of a reformatted sagittal CT image of the lower thoracic spine. There is a horizontal fracture through the spinous process and pedicles. There is also a compression fracture of the vertebral body. These types of injures are seen in impact injures where hyperflexion has occured with lap seatbelt injuries. It is also seen in certain types of falls. The most common symptom is back pain. Half of the patients with this type of injury also have serious blunt injury to their internal organs. These are usually lower level of t-spine so spinal cord injury is rare. However, spinal nerve damage is common resulting in bowel and bladder problems. Treatment of these fractures are done with immobilization and surgical fixation. This is a Sagittal MRI of a facet dislocation of C-7 on T1. Cervical fractures and/or dislocations occur when injuries applied to the cervical spine are greater than the strength of the vertebral bodies or the the supporting ligaments. Subluxation or dislocation occur when there is a disruption in the posterior soft tissue supporting ligaments. These can occur with or without neurologic injury, depending on the extent . Sometimes the initial diagnosis is made by plain radiographs of the lateral c-spine in flexion and extension. This should only be done in the presence of a spine surgeon and in a patient who is awake.
This is a Sagittal MRI of a facet dislocation of C-7 on T1. Cervical fractures and/or dislocations occur when injuries applied to the cervical spine are greater than the strength of the vertebral bodies or the the supporting ligaments. Subluxation or dislocation occur when there is a disruption in the posterior soft tissue supporting ligaments. These can occur with or without neurologic injury, depending on the extent . Sometimes the initial diagnosis is made by plain radiographs of the lateral c-spine in flexion and extension. This should only be done in the presence of a spine surgeon and in a patient who is awake. 







